When it comes to union activity in healthcare, registered-nurse organizing campaigns and strikes dominate the headlines. At Chicago’s Rush University Medical Center, 1,830 RNs voted to join National Nurses United in May. The Teamsters have made clear their mission to unionize Michigan nurses, so they can wage disruptive strikes like the one at Grand Blanc’s Henry Ford Genesys Hospital, where around 600 RNs have been on strike since Sept. 2025. And everyone watching healthcare noticed this year’s NYSNA strike that was costly for workers along with their employers.
So yes, RN-based union activity attracts the most attention, but we couldn’t resist digging beyond those headlines. We recently used LRIrightnow data to show why 2025’s 88% healthcare union win rate is more complicated than it seems, and how this sector’s small-unit trend illustrates a key union strategy. Now it’s time to dispel the media myth that RNs make up the majority of healthcare organizing activity. The data shows that employers have a vulnerability gap worth closing in this industry.
Non-RN Petitions Are The Majority, And This Isn’t New
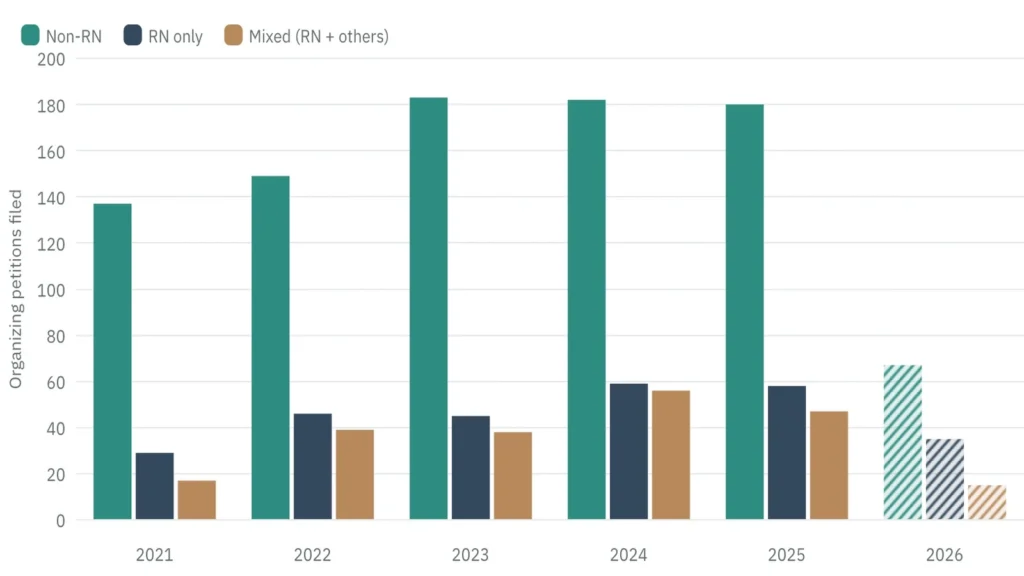
LRIrightnow graph data representation on organizing units that are non-RN, RN-only, and mixed
Looking at the total number of healthcare union petitions is telling. Across 1,843 union-filed organizing petitions in healthcare from January 2021 through early June 2026, RN-only units are consistently outnumbered by non-RN units, and mixed units with some RNs, in every single year. 2026 is shaded out due to being a partial year, but it still follows this same pattern.
These numbers cover hospitals, skilled nursing and residential care, and ambulatory settings, and they exclude decertification petitions and employer-filed cases. For the past five years, non-RN units made up the majority of healthcare organizing petitions, ranging from 57 to 75 percent each year. In the peak year, 2024, 59 petitions were RN-only, 182 were non-RN units, and 56 mixed units combined RNs and other roles.
Who are those non-RN workers? Technical staffers, lab workers, clerks, housekeepers, drivers, food-service workers, and other medical professionals. Some nursing aides are also included, but technical and service staff outnumber any nursing-adjacent role.
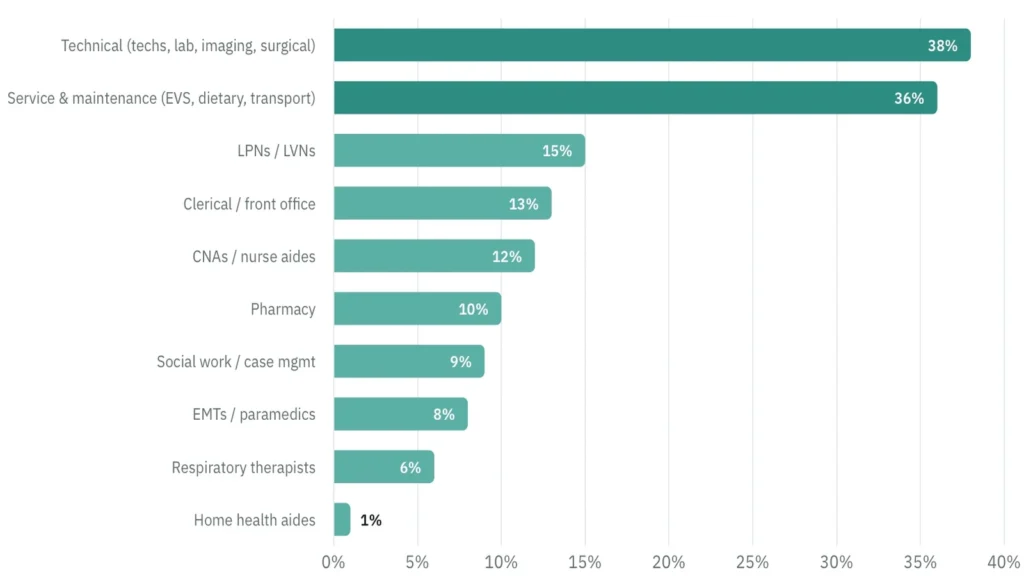
LRIrightnow data graph on organizing roles in healthcare union petitions
What This Means for Employers
There’s a lesson here, which is that labor relations strategies that are geared only toward organizing nurses leave healthcare employers vulnerable to the risk of unions targeting many other roles.
There is also a procedural wrinkle to consider, and it’s rarely triggered by RN-only campaigns. Under Section 9(b)(1) of the National Labor Relations Act, the Board cannot include professional and non-professional employees in the same unit unless the professional employees vote to join it first. When a non-RN petition covers a mix of both, a separate vote is necessary, which changes who participates, what the resulting unit looks like, and what arguments the employer can raise during the process. Employers that have only thought through RN-only scenarios tend to get caught flat-footed when those situations come up.
Other blind spots exist, too. In our experience, vulnerability assessments almost always focus on nursing, which means the technical, service, and support staff receive the least attention. And for multi-site healthcare systems, employers should consider every location in addition to flagship hospitals while weighing union exposure for non-RN workforces.
The tech, the aide, the housekeeper, the dietary worker: those campaigns have outnumbered RN filings every year for five years. Big Labor is not limiting its healthcare targets to the nursing station. Preparing for one role in a hospital leaves employers unprepared for the rest.